
Strategic Synthesis Of ASGCT And ASCO 2026
By Johnathon Anderson, Ph.D.

The spring 2026 conference season made one thing obvious to those of us watching the data: the artisan era of ex vivo cellular manufacturing is finally receding. We saw the technological architecture laid out at the American Society of Gene and Cell Therapy (ASGCT) meeting. Weeks later, the American Society of Clinical Oncology (ASCO) provided the hard clinical evidence that these platforms actually work in human patients.
With an aggregate $16 billion in Big Pharma capital deployed industrywide over just 13 months, our sector has officially shifted out of preclinical speculation. Having managed clinical operations, guided translational pipelines, and navigated the regulatory hurdles of biotech startups firsthand, I can tell you this isn't just theory anymore. Investors, CMC leaders, and C-suite executives are done rewarding incremental "me too" designs targeting rodent B cell depletion. Capital is now filtering for one thing: the ability to disrupt the operational logistics and cost of goods sold (COGS) of cell therapy.
The Strategic Hedge: Big Pharma’s Commercial Filter
Eli Lilly’s recent acquisition strategy is the perfect lens for this shift. Within the $16 billion industrywide pool, Lilly's $9.4 billion dual acquisition strategy illustrates a deliberate corporate hedge across our field’s central mechanistic dilemma: stable genomic integration vs. the safety and re-dosability of transient expression. These acquisitions act as a harsh commercial filter, separating platforms by their capacity to solve real-world clinical bottlenecks.
The Viral, Stable Integration Bet
Take Lilly’s $7 billion buyout of Kelonia Therapeutics. Kelonia’s in vivo gene placement system (iGPS) uses engineered lentiviral vectors (LVVs) for stable CAR integration. We saw the rationale at ASCO: a 100% overall response rate (ORR) and MRD-negative bone marrow in all evaluable myeloma patients at one month. For discovery scientists, the resolution of that diagnostic tool matters; this MRD-negative status was evaluated via highly sensitive assays (such as next-generation sequencing or flow cytometry) with rigorous 10⁻⁵ or 10⁻⁶ sensitivity thresholds, cementing the clinical de-risking event.
But the real headline for CMC strategists? Kelonia achieved this with a 13-day median turnaround time from consent to infusion. Thirteen days. Let that sink in. For an off-the-shelf in vivo biologic, this 13-day window is not a manufacturing delay; it accounts for mandatory clinical staging, including patient screening, insurance authorizations, and lymphodepletion conditioning regimens prior to infusion. By eliminating the bespoke patient apheresis and centralized production steps, we are finally bypassing the weeks of anxiety, batch failures, and slot availability nightmares that have bottlenecked CAR-T for a decade.
The Nonviral, Transient Bet
Then there is the other side of the hedge. Lilly’s $2.4 billion acquisition of Orna Therapeutics secures a premier nonviral platform built on circular RNA (circRNA) and lipid nanoparticles (LNPs). For solid tumors and autoimmune conditions, prolonged viral integration carries risks we don't always need to take. The Orna platform provides a transient, titratable pharmacokinetic profile. It acts as a mandatory safety valve against prolonged on-target, off-tumor toxicities.
Engineering Precision Biodistribution: Solving The Tropism Bottleneck
With Kelonia setting a 13-day operational benchmark, the race for market dominance comes down to precision biodistribution. Emerging platforms must prove that their delivery vehicles can bypass natural broad tropism and dodge innate immune clearance. To balance systemic survival with cell-specific entry, developers are addressing homing and immune evasion as distinct engineering challenges.
Next-Generation Lentiviral Engineering (Cellular Homing vs. Systemic Survival)
To get targeted in vivo transduction without off-target genotoxicity, developers are rapidly moving away from traditional single-chain variable fragments (scFvs). Chengdu Origen Biotechnology and PersonGen BioTherapeutics are leveraging VHH single-domain antibodies (nanobodies) for precise CD7 retargeting. From an operational perspective, VHH domains are a massive upgrade. They offer superior conformational stability and reduced steric hindrance compared to scFvs, allowing for high-density functionalization on the viral envelope without wrecking titer yields.
Once homing is solved, the next operational hurdle is systemic survival, specifically overcoming complement-mediated inactivation. The Fred Hutch Cancer Center tackled this directly by showcasing cocal-pseudotyped LVs, which exhibit significantly lower preexisting serum neutralization in human cohorts than our standard VSV-G envelopes.
The LNP Revolution (Hepatic Evasion And Avidity)
Nonviral delivery completely bypasses the complex CMC logistics of viral manufacturing. But historical LNP platforms frequently failed due to rapid ApoE-mediated clearance and the resulting liver sink. Nava Therapeutics’ NT-001 candidate solves this via an "immunotropic" ionizable lipid, tuned specifically to minimize hepatic biodistribution.
Stanford University took a different route, presenting a dual protein-conjugated LNP combining anti-CD5 targeting with IL-7 functionalization. This dual-ligand approach exploits binding "avidity" to physically force nanoparticle adherence to target T cells. While this avidity strategy is highly potent, the ongoing pharmacological challenge is fine-tuning the stoichiometric ratios of these ligands. Because the IL-7 receptor signals through the common gamma chain (CD132), which is broadly expressed across multiple hematopoietic lineages, precise calibration is required to ensure the LNPs do not inadvertently engage and transfect off-target immune compartments.

Payload Innovations: The "Genetic Rheostat"
Stable integration works beautifully for aggressive hematological cancers. Managing toxicities in broader indications, however, requires precise mechanisms of control.
Extended Yet Finite Expression And Spatial Gating
Circular RNA (circRNA) has emerged as the baseline for nonviral payloads because it resists rapid exonuclease degradation. While circRNA is non-integrating, its core pharmacological advantage is that it is less transient than linear mRNA. It provides an "extended yet finite" expression window, delivering the prolonged exposure needed to achieve therapeutic thresholds without the lifelong safety liabilities of permanent genomic integration.
To optimize this, Strand Therapeutics is pairing circRNA with its proprietary Signal Lock technology. It is critical to uncouple the terminology here: the circRNA platform itself dictates the temporal control via dosing intervals, while the Signal Lock acts as a spatial firewall. By engineering lineage-specific microRNA (miRNA) target sites into the untranslated regions, the payload automatically triggers RISC-mediated degradation if it inadvertently hits off-target tissues like the liver. This provides spatial restriction, effectively preventing hepatic genotoxicity.
Permanent Rewriting Without DSBs
For curative oncology applications, we need persistent CAR populations without the genotoxicity of undirected Cas9 double-strand breaks (DSBs). Azalea Therapeutics is pioneering CRISPR biomimicry to knock the CAR construct directly into the endogenous TRAC locus, placing it under natural promoter regulation to delay exhaustion. Tessera Therapeutics’ RNA Gene Writer technology effectively writes the CAR sequence directly into the genome via mobile genetic elements.
At the same time, Kano Therapeutics and CPTx GmbH are utilizing circular single-stranded DNA (ssDNA) templates. Because single-stranded DNA templates lack the double-helical structure required to activate sequence-independent dsDNA sensors like cGAS, they cleanly evade the cGAS-STING pathway, bypassing the interferon-mediated toxicities that routinely compromise double-stranded templates.
Market Diversification: Solid Tumors And The Autoimmune Reboot
Now that the delivery chassis and payload architectures are seeing clinical validation, developers are aiming at the field's most lucrative, and difficult, targets: systemic autoimmune diseases and the highly immunosuppressive tumor microenvironment (TME).
The Autoimmune Reboot
Traditional monoclonal antibodies like rituximab deplete circulating B cells but routinely miss deeply tissue-resident memory B cells. The result is inevitable disease relapse. In vivo generated CD19 CAR T cells actively penetrate secondary lymphoid organs to completely ablate the autoreactive humoral compartment. Nava Therapeutics is positioning its transient LNP platform here to achieve deep B cell depletion and then naturally decay. While transient platforms may necessitate cyclic redosing protocols to guarantee full tissue-resident ablation, the mitigation of lifelong aplasia risks presents a vastly superior therapeutic index for nonmalignant indications.
Breaching The TME Via Innate Immunity
As an industry, we have spent years watching alpha-beta T cells struggle against the physical stroma barriers and hypoxia of solid tumors. To breach the TME, companies are expanding in vivo transduction to the innate immune compartment.
It is vital to note that while the core genetic payload cassette is highly modular when targeting a consistent immune lineage, expanding across different cell types (e.g., from T cells to myeloid lineages) demands a concurrent re-engineering of the vehicle's surface tropism properties. Navigating this biological hurdle, Ensoma and Modulari-T Bioscience are generating CAR-myeloid and CAR-natural killer (NK) cells in vivo. Macrophages naturally traffic into solid tumors. Arming them with CARs allows for direct phagocytosis and active-matrix remodeling, while CAR-NK cells provide potent cytotoxicity with a much lower risk of severe CRS.
The Post-Preclinical Era: Disrupting CMC And COGS
Looking at the combined data from ASGCT and ASCO 2026, the reality is stark. Exceptional preclinical efficacy in murine models will no longer secure late-stage capitalization. We have entered an era dictated by clinical pharmacology, GLP toxicology, and translational rigor.
Moving forward, theoretical debates over vector tropism will be superseded by hard Phase 1 pharmacodynamic readouts and the ability to survive the IND bottleneck. The developers who win will be the ones who fundamentally disrupt the CMC landscape.
In my experience, the true commercial promise of in vivo CAR-T isn't just the science. It is the transition of cellular therapy from a bespoke facility-bound autologous process into standard highly scalable biologics fill/finish logistics. Achieving this scalability relies heavily on advanced formulation science to keep notoriously fragile LNPs and LVVs viable on a commercial scale. Success here demands precise excipient strategies, such as utilizing mannitol to stabilize the complex lipid and protein structures during lyophilization or freezing. By solving these formulation bottlenecks, slashing COGS, and eliminating supply chain delays, we can finally dismantle the six-figure price tags gating patient access. Kelonia’s clinical maturity proves this operational pivot isn't just a talking point on a pitch deck. It is already happening.
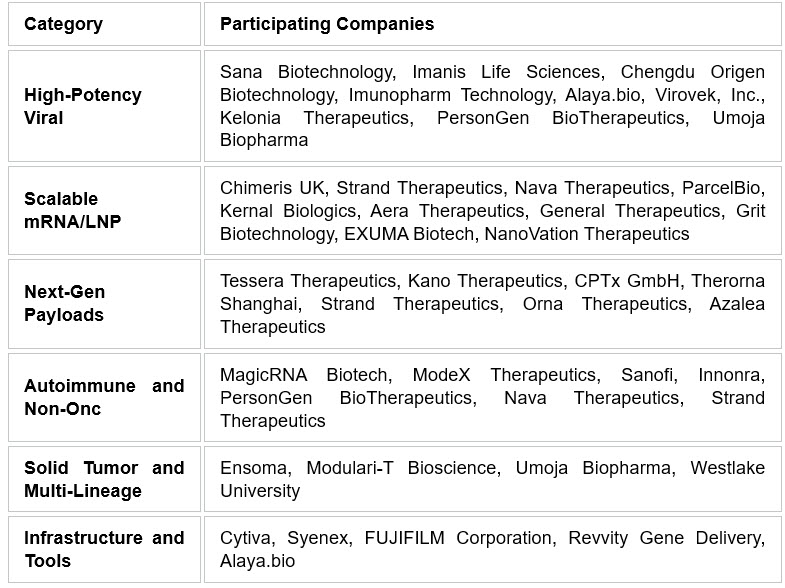
Summary Of Key Commercial Players (ASGCT/ASCO 2026)
About The Author
 Johnathon Anderson, Ph.D., is an associate professor and scientific program officer at the UC Davis School of Medicine, specializing in the translational development and commercialization of advanced cell and gene therapies. As a former biotech cofounder and strategic consultant, Anderson advises emerging startups and principal investigators on operational scaling, advanced funding mechanisms, and the clinical industrialization of next-generation therapeutic platforms.
Johnathon Anderson, Ph.D., is an associate professor and scientific program officer at the UC Davis School of Medicine, specializing in the translational development and commercialization of advanced cell and gene therapies. As a former biotech cofounder and strategic consultant, Anderson advises emerging startups and principal investigators on operational scaling, advanced funding mechanisms, and the clinical industrialization of next-generation therapeutic platforms.